Intro – Mediterranean Diet throughout History
Mediterranean Diet has its origin in adjacent regions to the Mediterranean Sea basin, a place with distinctive environmental characteristics and played a relevant role in humanity history. Some historians call this geographical area “the cradle of society” due to its relevance during ancient world development. Mediterranean regions were a meeting place that enabled several cultures to interact. Civilizations exchanged customs, lifestyles, languages and beliefs, which were changing and transforming over the time, from Cretans, Phoenicians, Greeks to Romans (1).
Agriculture had a key role, being cereals and vegetables the most available foods. Whereas animal foods were less frequent than fish and seafood, especially in the recipes from richer population. Bread, wine, olives and olive oil were the most habitual foods (2). Mediterranean Diet has been continuously evolving; different people influenced and contributed with novel foods that enriched this dietary pattern. Mediterranean Diet has been also influenced by German people, who were mainly nomads, hunters and farmers (3). Arab people also contributed with some key foods such as spices, which are highly appreciated, and plant-based vegetables such as aubergines, almonds, oranges, lemons and pomegranates (4). In addition, the discovery of America represented an important ephemerid that brought a wide range of unknown foods (e.g. potatoes, tomatoes, peppers, corn and new varieties of beans (5). Those foods are now part of the foundations of the Mediterranean Diet.
Currently, traditional Mediterranean Diet is usually described such as diet in Crete, Greece and regions in the south of Italy at the beginning of the 1960s. However, Spanish, Italian, Moroccan, French, Lebanese, Turkish, Portuguese and other Mediterranean countries diets have similarities in their composition. In addition, this food pattern is accompanied by regular physical activity (6).
In 2013, United Nations Educational, Scientific and Cultural Organization (UNESCO) recognized the Mediterranean Diet as a part of Human Culture and Intangible Cultural Heritage.
Mediterranean Diet goes beyond to be only an exceptional dietary pattern; it also involved life-style, a Mediterranean dynamic cultural complex, which include traditions concerning to agriculture, fishing and livestock, food processing, preservation, cooking techniques, food sharing and consumption. Cooking and meals are perfect social meetings to exchange ideas and communicate with family, friends and neighbours, to forge closer ties, in cordiality and respect. The Mediterranean Diet has a main role in culture, being present in festivities, celebrations and daily life, represented in crafts, in markets, as places for exchange, or inside familiar nucleus, where techniques and recipes are transmitted.
Dietary intake and food pattern play a relevant role in human health. However, the link between the Mediterranean Diet and health was not described until 1960, after that some scientific results were available. The American physiologist Ancel Keys and his colleagues published the Seven Countries study (6), an observational study that showed the relationship between the Mediterranean dietary pattern and its protective effect against coronary heart disease and cardiovascular mortality. This study linked by the first-time saturated fat acids intake and high fasting total cholesterol blood levels with coronary heart disease mortality in different populations. Similar results were subsequently observed by the MONICA (Multinational Monitoring of Trends and Determinants in Cardiovascular Disease) program (7) which collected data about total mortality and mortality from heart disease in 26 countries between 1950 and 1978. Data permitted to observe a north-south gradient, so that North countries had a higher cardiovascular disease-related mortality than South countries. Moreover, it has been noted that Mediterranean Diet is present in certain regions so-called Blue Zones (Sardinia in Italy and Icaria in Greece), which are distinguished by their life expectancy and quality of life (8).
Over the last several decades, scientific evidence has related Mediterranean Diet adherence with health benefits in blood lipids concentration, blood pressure, insulin resistance, arterial stiffness, oxidative stress, lower cardiovascular risk and a better evolution of diabetes and cardiovascular diseases (9–11). This has contributed to its recognition such as a healthy diet by several international organizations. Since 2010, American Dietary Guidelines included Mediterranean eating pattern style as an example of a healthy diet (12,13), but also traditional Mediterranean Diet has been introduced in gastronomy because of its ingredients and tasty key foods.
This document review knowledge and scientific evidence about the Mediterranean Diet, focusing on the general understanding about Mediterranean Diet characteristics, analyzing their principal food components and the Mediterranean Diet and health link. Moreover, partners’ countries Mediterranean Diet adherence is evaluated and their association with health parameters is described.
In addition, it has been considered necessary to group the data from the different food composition tables in each country considering they are indispensable tools to carry out a proper nutritional assessment of food. The differences between the tables are variable depending on the bibliographic sources consulted, the natural variability of the food (animal feed, soil fertilization, ripeness, region of origin, etc.), technological treatments, sampling methods and several other factors. Another relevant tool to highlight were the different graphic representations of their national recommendations on healthy nutrition, which is an efficient way to assure that the information provided in the different nutritional food guides is easier to understand, and it was interesting to learn how each country represented and transmitted it.
References
- Braudel F, Duby G, Gatto L. Il Mediterraneo : lo spazio e la storia, gli uomini e la tradizione. Newton Compton; 2002.
- Montanari M, Devroey J-P. Il mondo in cucina : storia, identità, scambi. Laterza; 2002.
- Montanari M. Convivio : storia e cultura dei piaceri della tavola dall’Antichitá al Medioevo. Ed. Laterza; 1989.
- Tannahill R. Storia del cibo. Rizzoli; 1987.
- Montanari M. La fame e l’abbondanza : storia dell’alimentazione in Europa. Laterza; 1997.
- Keys A AC, Blackburn H, Buzina R, Djordjević BS, Dontas AS, Fidanza F, et al. Seven countries: a multivariate analysis of death and coronary heart disease. Cambridge: Harvard University Press; 1980. p. 381.
- Thom TJ, Epstein FH, Feldman JJ, Leaverton PE. Trends in total mortality and mortality from heart disease in 26 countries from 1950 to 1978. Int J Epidemiol. 1985 Dec;14(4):510–20.
- Blue Zones Project [Internet]. Minneapolis, MN: Blue Zones. 2013. Available from: http://www.bluezones.com/
- Estruch R, Ros E, Salas-Salvadó J, Covas M-I, Corella D, Arós F, et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet. N Engl J Med. 2013 Apr 4;368(14):1279–90
- Serra-Majem L, Roman B, Estruch R. Scientific Evidence of Interventions Using the Mediterranean Diet: A Systematic Review. Nutr Rev. 2006 Feb;64(2 Pt 2):S27–47.
- Lorgeril M de, Salen P. Dietary Prevention of Coronary Heart Disease: The Lyon Department of Agricuture U, Department of Health U, Services H. Dietary Guidelines for Anericans 2010 – DietaryGuidelines. 2010.13. U.S.
- Department of Health and Human Services and U.S. Department of Agriculture. 2015 – 2020 Dietary Guidelines for Americans: Eight Edition.
- S. Department of Health and Human Services and U.S. Department of Agriculture. 2015.
Plant-based foods are the main constituents of the Mediterranean Diet. This dietary pattern is rich in fruits, vegetables, beans, legumes and whole grains cereals, with complex carbohydrates. Nuts and seeds are also present in daily intake. Moreover, it is also rich in monounsaturated fatty acids due to olive oil, which is a key food of Mediterranean Diet and it is used for all cooking and dressing techniques. While animal origin foods intake is less relevant, dairy foods consumption is low or moderate, mainly fermented milks like yogurt and cheese, which are recommended daily. On the one hand, fish, seafood and lean meat intake are present in diet around twice per week. Eggs consumption is also moderate, whereas red meat and processed meat intake is limited, less than once per week. On the other hand, it is common to accompany food intake with moderate wine drinking during meals. Mediterranean Diet also stands out for its spices richness, which strength its organoleptic qualities, mainly smell and taste, outside adding salt or fat. Another added value is that the ingredients used in characteristic Mediterranean recipes are mainly seasonal, grown or produced locally and they are minimally processed. Moreover, seasonal fruits are the most common daily desserts, promoting a reduction in simple sugar presence (1,2).
Beyond foods that make up Mediterranean Diet, it is based on social harmony and family time, daily meetings around the table, special events and festivities sharing the cooking time and traditional recipes, which passed down through families. Therefore, Mediterranean Diet is a life-style, within the framework of an active life, including work, outdoor leisure activities and adequate rest.
From the nutritional point of view, in traditional Mediterranean Diet, total fats represent approximately a 25-35% of daily energy intake and only 7-8% of it is saturated fat acids, being scarce in animal fats. By contrast, it is rich in monounsaturated fatty acids. As well, it has an adequate Healthy omega-6 and omega-3 fatty acids ratio. Regarding to carbohydrates content, they are mainly complex carbohydrates, with a minor presence of simple sugars. The characteristic plant origin foods content makes Mediterranean Diet rich in fiber, vitamins, minerals and in phytochemical compounds, which are present in small quantities and provide antioxidant among other health benefits (3).
References
- Shen J, Wilmot KA, Ghasemzadeh N, Molloy DL, Burkman G, Mekonnen G, et al. Mediterranean Dietary Patterns and Cardiovascular Health. Annu Rev Nutr. 2015 Jul 17;35(1):425–49.
- Trichopoulou A, Bamia C, Trichopoulos D. Anatomy of health effects of Mediterranean diet: Greek EPIC prospective cohort study.
- Zamora-Ros R, Serafini M, Estruch R, Lamuela-Raventós RMM, Martínez-González MAA, Salas-Salvadó J, et al. Mediterranean diet and non enzymatic antioxidant capacity in the PREDIMED study: Evidence for a mechanism of antioxidant tuning. Nutr Metab Cardiovasc Dis. 2013 Dec;23(12):1167–74.
Fruits and vegetables are the basis of Mediterranean Diet. These are present in a high variety in almost all recipes of traditional cuisine. Equally, they can be eaten raw or cooked and this is particularly beneficial given that food nutrients, micronutrients and minority compound levels vary depending on cooking temperature and procedures (1). Although, nowadays vegetables and fruits are available annually thanks to the development of new growing and crop techniques and globalization. Despite the fact that food industry enhanced unsustainable crop, Mediterranean Diet is featured by nearby products and seasonality. For that reason, fruits and vegetables are varied and vary during the year. Regarding to that, it is difficult to detail all fruits and vegetables in Mediterranean Diet, however, some of them are summarized in table 1.
Table 1 – Fruits and vegetables in Mediterranean Diet
| Fruits | Vegetables |
| Orange, mandarin, apple, pears,
strawberries, grapes, dates, figs, melons, watermelons, peaches, apricots, nectarines, lemons, cherries, pomegranates, blueberries, plums, etc. |
Tomatoes, potatoes, onions, scallions,
garlic, carrots, cucumber, peppers, zucchinis, broccoli, cabbage, Brussels sprouts, spinach, chard, artichokes, lettuce, beets, aubergines, pumpkin, radishes, turnips, sweet potatoes, asparagus, chicory, etc. |
Fruits and vegetables have high water content and provide to diet macronutrients, micronutrients and phytochemicals (e.g. natural bioactive compounds with antioxidant proprieties, among other). Fruits highlight by their contribution of potassium and vitamin C intake, and vegetables are sources of vitamin A, C, K, E, B1, B3, B6, choline and minerals such as potassium, copper, folate, magnesium, iron, manganese and leaf vegetables contribute with carotenoids, vitamin A, C, E, folate, iron and calcium intake. Moreover, fruits and vegetables are one of the main sources of dietary fiber and phytochemicals compounds, which are liked with healthier status (2–4).
Fruit and vegetable intake have been related with several health benefits. A high consumption is associated with reduced risk of hypertension, cardiovascular heart disease and stroke, additionally to a probable cancer risk reduction when fruit and vegetables intake is high, especially during the exposure to carcinogens, such us smokers. On one hand, it seems to be enough scientific evidence that support the anti-obesogenic role of fruits and vegetables, due to its potential preventive effect on body weight gain by contributing to weight stability, because their intake usually substitutes calorie-rich products (5). On the other hand, overweight and obesity are key risk factors in type 2 diabetes development, so an abundant intake of fruits and vegetables might be inversely related with diabetes type 2 incidence; however, no direct associations had been observed. In addition, dementia, osteoporosis, some degenerative ocular diseases, respiratory diseases (such as asthma, chronic obstructive pulmonary disease (COPD)) and rheumatoid arthritis are pathologies that showed favorably response to fruit and vegetable intake (6).
References
- Da Silva R, Bach-Faig A, Raidó Quintana B, Buckland G, Vaz de Almeida MD, Serra-Majem L. Worldwide variation of adherence to the Mediterranean diet, in 1961–1965 and 2000–2003. Public Health Nutr. 2009 Sep 1;12(9A):1676–84.
- Food Composition Databases Show Foods List [Internet]. [cited 2019 Apr 15]. Available from: https://ndb.nal.usda.gov/ndb/search/list
- Slavin JL, Lloyd B. Health Benefits of Fruits and Vegetables. Adv Nutr. 2012 Jul
1;3(4):506.
- Liu RH. Health-Promoting Components of Fruits and Vegetables in the Diet.
Adv Nutr. 2013 May 1;4(3):384S-392S.
- Schlesinger S, Neuenschwander M, Schwedhelm C, Hoffmann G, Bechthold A,
Boeing H, et al. Food Groups and Risk of Overweight, Obesity, and Weight
Gain: A Systematic Review and Dose-Response Meta-Analysis of Prospective
Studies. Adv Nutr. 2019 Mar 1;10(2):205–18.
- Boeing H, Bechthold A, Bub A, Ellinger S, Haller D, Kroke A, et al. Critical review: vegetables and fruit in the prevention of chronic diseases. Eur J Nutr. 2012
Sep;51(6):637–63.
Whole grains offer higher health benefits than refined grains, which are stripped of valuable nutrients in the refining process. Grain kernels contain three parts, the bran, germ and endosperm. In the late 19th century, it changed the way to process grains. Milling leaves only the soft, easy-to-digest endosperm, and strips away the bran and the germ. Without the fibrous bran, the grain is easier to chew. The germ is removed because of its fat content, which can limit the shelf life of processed wheat products. The resulting highly processed grains are much lower in nutritional quality, since process strips away more than half of B vitamins, almost all vitamin E, and virtually all of the fiber. Although some nutrients may be added back by fortification, other health- promoting components of whole grains cannot be replaced (1).
Some academic and industry consortium, like the Health Grain Forum, have suggested that the food labelled as “whole grain” should contain more than 30% of whole-grain ingredients, and more whole grain than refined grain ingredients, based on its dry-weight (1). An easy way to tell if a food product is high in 100% whole grains is to make sure it is listed first or second in the ingredient list. Or better yet, choose unprocessed whole grains: 1. Amaranth; 2. Kamut; 3. Spelt; 4. Barley; 5. Millet; 6. Wild Rice; 7. Brown Rice; 8. Quinoa; 9. Triticale; 10. Buckwheat; 11. Rye; 12. Bulgur; 13. Oat; 14 Corn; and 15. Sorghum.
The 2015-2020 Dietary Guidelines for Americans from the Department of Agriculture of US Government recommends eating 85 g (6 ounces) of grain foods daily and getting at least half of that grain intake from 100% whole grains (2). However, due to an increasing amount of research showing the various health benefits derived from whole grains, and even a possible detrimental effect when eating mostly refined grains, the recommendation is to choose mostly whole grains instead of refined grains. Denmark, in Europe, recommend the consumption of at least 75 g/day (3), whereas the Mediterranean diet pyramid recommends the consumption of one or two servings of cereals (20 to 40 g) at each main meal (in the form of bread, pasta, rice, couscous and others), preferably whole grain (4).
Whole grain kernels contain the three parts, the bran, germ, and endosperm. The bran is the fiber-rich outer layer that supplies B vitamins, iron, copper, zinc, magnesium, and several phytochemicals, that have key role in disease prevention. The germ is the core of the seed and it is rich in healthy fats, vitamin E, B vitamins, and also phytochemicals. The endosperm is the interior layer that holds carbohydrates, protein, and small amounts of B vitamins and minerals. Refined grains lack of bran and endosperm, and only maintain the core of the seed.
Nowadays, all researchers consider that in the relationship between carbohydrates and health the quality of the carbohydrates is as important as the quantity. Most of the studies performed have shown a connection between whole grains and better health, although the absence of a universally accepted definition of “whole grain” difficult to study its consumption in any population.
Mortality: A meta-analysis combining results from studies conducted in the U.S., the United Kingdom, and Scandinavian countries (which included health information from over 786,000 individuals), found that people who ate 70 grams/day of whole grains—compared with those who ate little or no whole grains—had a 22% lower risk of total mortality, a 23% lower risk of cardiovascular disease mortality, and a 20% lower risk of cancer mortality (5).
Cardiovascular Disease: Eating whole grains instead of refined grains lowers plasma total cholesterol, low-density lipoprotein (LDL) cholesterol, triglycerides, and insulin concentrations. A meta-analysis of seven major studies showed that cardiovascular disease (heart attack, stroke, or the need for a procedure to bypass or open a clogged artery) was 21% less likely in people who ate 2.5 or more servings of whole-grain foods a day compared with those who ate less than 2 servings a week (6).
Diabetes: Replacing refined grains with whole grains and eating at least 2 servings of whole grains daily may help to reduce type 2 diabetes risk. The fiber, nutrients, and phytochemicals in whole grains may improve insulin sensitivity and glucose metabolism and slow the absorption of food, preventing blood sugar spikes. In contrast, refined grains tend to have a high glycemic index and glycemic load with less fiber and nutrients. In a study of more than 160,000 women whose health and dietary habits were followed for up to 18 years, those who averaged 2 to 3 servings of whole grains a day were 30% less likely to have developed type 2 diabetes than those who rarely ate whole grains. When the researchers combined these results with those of several other large studies, they found that eating an extra 2 servings of whole grains a day decreased the risk of type 2 diabetes by 21% (7).
Cancer: The data on cancer are mixed, with some studies showing a protective effect of whole grains and others showing none. Thus, a large five-year study among nearly 500,000 men and women suggests that eating whole grains, but not dietary fiber, offers modest protection against colorectal cancer (8). By contrast, a review of four large population studies also showed a protective effect of whole grains from colorectal cancer, with a cumulative risk reduction of 21% (9).
References
- Ross AB, van der Kamp J-W, King R, Lê K-A, Mejborn H, Seal CJ, et al. Perspective: A Definition for Whole-Grain Food Products-Recommendations
from the Healthgrain Forum. Adv Nutr. 2017 Jul;8(4):525–31.
- S. Department of Health and Human Services and U.S. Department of Agriculture. 2015 – 2020 Dietary Guidelines for Americans: Eight Edition. U.S.
Department of Health and Human Services and U.S. Department of Agriculture. 2015.
- Frølich W, Aman P, Tetens I. Whole grain foods and health – a Scandinavian
perspective. Food Nutr Res. 2013 Jan 19;57(1):18503.
- Bach-Faig A, Berry EM, Lairon D, Reguant J, Trichopoulou A, Dernini S, et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011 Dec 13;14(12A):2274–84.
- Zong G, Gao A, Hu FB, Sun Q. Whole Grain Intake and Mortality From All Causes, Cardiovascular Disease, and Cancer. Circulation. 2016 Jun 4;133(24):2370–80.
- Mellen PB, Walsh TF, Herrington DM. Whole grain intake and cardiovascular disease: A meta-analysis. Nutr Metab Cardiovasc Dis. 2008 May;18(4):283–90.
- de Munter JSL, Hu FB, Spiegelman D, Franz M, van Dam RM. Whole Grain, Bran, and Germ Intake and Risk of Type 2 Diabetes: A Prospective Cohort Study and Systematic Review. Groop LC, editor. PLoS Med. 2007 Aug 28;4(8):e261.
- Strayer L, Jacobs DR, Schairer C, Schatzkin A, Flood A. Dietary carbohydrate, glycemic index, and glycemic load and the risk of colorectal cancer in the BCDDP cohort. Cancer Causes Control. 2007 Oct;18(8):853–63.
Aune D, Chan DSM, Lau R, Vieira R, Greenwood DC, Kampman E, et al. Dietary fibre, whole grains, and risk of colorectal cancer: systematic review and dose-response meta-analysis of prospective studies. BMJ. 2011 Nov 11;343(nov101): d6617–d6617.
Olive oil is a key component of the Mediterranean Diet, being the main source of vegetable fat, especially monounsaturated fatty acids (MUFA). According to the International Olive Council, there are five different types of olive oil: i. Extra Virgin Olive Oil; ii: Virgin Olive Oil; iii: Refined Olive Oil; iv: Olive Pomace Oil and v. Lampante Oil.
Extra Virgin Olive Oil (EVOO) is the best olive oil and it is very precise regards production methods, taste and chemical composition. EVOO must come from the first pressing of fresh olives, normally within 24 hours of harvesting, must be extracted by non-chemical, mechanical means, and without the use of excessive heat, the free fatty acid or acidity level must be less than 0.8% and it must be defect free – having a perfect taste and aroma. It contains multiple bioactive and antioxidant components, such as polyphenols, phytosterols and vitamin E (1). Virgin olive oil also comes from the first pressing and must have an acidity level of less than 2% therefore it is of inferior quality to Extra Virgin Olive Oil. It is flavour intensity can vary and its taste is milder than EVOO.
In contrast, some olive oils are refined by using agents such as acids, alkalis, and heat to extract as much oil as possible from the olive pulp that remains after the first pressing. The result is a fattier and more acidic oil which lacks taste, aroma and natural antioxidants. This is why producers need to add unrefined Extra Virgin or Virgin Olive Oil to impart some of flavour, colour and aroma into the blend. Since refined olive oil during the refining process loses phytochemicals, this oil is mixed with virgin olive oil to enhance the flavour, constituting the so-called common olive oil. The olive – pomace oil is the lowest grade of olive oil and it is made from the by-products of EVOO production. It is bland and extremely low in antioxidants. The lampante oil has severe defects, usually from bad fruit or poor processing practices. It is not fit for human consumption until it has been refined. Finally, the rapeseed oil obtained from canola is one of the oldest known vegetable oil that is also rich in oleic acid, but that differs in several other compounds with common olive oil (2).
Olive oil as a food and the Mediterranean Diet as a food pattern are associated with a decreased risk of cardiovascular disease, obesity, metabolic syndrome, type-2 diabetes and hypertension. A Mediterranean diet rich in olive oil and olive oil per se has been shown to improve cardiovascular risk factors, such as lipid profiles, blood pressure, postprandial hyperlipidemia, endothelial dysfunction, oxidative stress, and antithrombotic profiles. Although some of these beneficial effects can be attributed to the minor components of olive oil, it is very difficult to differentiate the effects of these components from those of the all fruit and even from the effects of the all diet, in this case, the Mediterranean diet (3).
All-cause mortality and cardiovascular mortality: Recent studies consistently support the concept that the OO-rich Mediterranean Diet is compatible with healthier aging and increased longevity. In the PREDIMED (PREvención con DIeta MEDiterránea trial, olive oil consumption, specifically the extra-virgin variety, was associated with reduced risks of cardiovascular disease and mortality in individuals at high cardiovascular risk. For each 10 g/d increase in extra-virgin olive oil consumption, cardiovascular disease and mortality risk decreased by 10% and 7%, respectively (4). Similarly, a lower risk of mortality was associated with regular consumption of olive oil in an Italian population after myocardial infarction and also in an elderly population. In the Spanish cohort of the European Prospective Investigation into Cancer and Nutrition (EPIC) study, total olive oil consumption has been associated with a decreased risk of coronary heart disease, and also all-cause and cardiovascular mortality (5). Thus, there is compiling evidences that olive oil consumption is associated with low all-cause and cardiovascular mortality.
Cardiovascular disease: Evidence suggests that olive oil intake is inversely associated with cardiovascular disease (CVD) in the Spanish general population and in a cohort of Italian women (3). A recent meta-analysis concluded that epidemiologic studies consistently found an inverse association between olive oil consumption and stroke, but there were inconsistencies between studies assessing coronary heart disease (CHD) as the end-point (6). Of note, most of the previous studies made no distinction among the different varieties of olive oil. However, several studies have found a greater beneficial effect in CHD and cardiovascular risk factors for the extra virgin olive oil variety than for the common variety (7). This distinction is important because EVOO contains much higher amounts of polyphenols than common olive oil. These polyphenols may have cardiovascular benefits beyond the lipid profile.
Diabetes: Demonstrated by dietary interventions in different population, olive oil consumption Improvement of glucose metabolism in normal subjects and patients with type 2 diabetes. Substitution of MUFA for SFA results in lower insulin requirement and plasma glucose concentrations, and is at least as effective as CHO. Two prospective studies from Southern European cohorts suggest a lower incidence of diabetes with increasing adherence to Mediterranean Diet in previously healthy persons or survivors of a myocardial infarction. In the PREDIMED trial, the arm of participants who followed a Mediterranean Diet supplemented with extra virgin olive oil showed a 40% reduction in the incidence of diabetes mellitus without significant changes in body weight (8).
Cancer: In countries where the population adheres to the Mediterranean Diet, such as Spain, Greece and Italy, and OO is the principal source of fat, rates of cancer incidence are lower than in northern European countries. Experimental and human cellular studies have provided new evidence on the potential protective effect of olive oil on cancer. Furthermore, results of case-control and cohort studies suggest that MUFA intake including olive oil is associated with a reduction in cancer risk (mainly breast, colorectal and prostate cancers) (4).
Other effects: Olive oil consumption may also have favorable effects on obesity, reduces age-related cognitive decline and incidence of Alzheimer’s disease (4).
In addition, different cohort and intervention studies have observed that olive oil consumption promotes of a less prothrombotic environment compared with SFA-rich diets, influencing different thrombogenic factors: reduction of platelet aggregation, thromboxane B2 production, von Willebrand factor (vWf), tissue factor, tissue factor pathway inhibitor, PAI-1, Factor VII and Factor XII. These latter effects may also help to explain the reduced incidence in myocardial infarction and stroke observed in subjects with higher consumption of olive oil in several cohort studies (4).
References
- COVAS M. Olive oil and the cardiovascular system. Pharmacol Res. 2007 Mar;55(3):175–86.
- Hoffman R, Gerber M. Can rapeseed oil replace olive oil as part of a Mediterranean-style diet? Br J Nutr. 2014 Dec 14;112(11):1882–95.
- López-Miranda J, Pérez-Jiménez F, Ros E, De Caterina R, Badimón L, Covas MI, et al. Olive oil and health: Summary of the II international conference on olive oil and health consensus report, Jaén and Córdoba (Spain) 2008. Nutr Metab Cardiovasc Dis. 2010 May;20(4):284–94.
- Guasch-Ferré M, Hu FB, Martínez-González MA, Fitó M, Bulló M, Estruch R, et al. Olive oil intake and risk of cardiovascular disease and mortality in the PREDIMED Study. BMC Med. 2014 Dec 13;12(1):78.
- Buckland G, Mayén AL, Agudo A, Travier N, Navarro C, Huerta JM, et al. Olive oil intake and mortality within the Spanish population (EPIC-Spain). Am J Clin Nutr. 2012 Jul;96(1):142–9.
- Martínez-González MA, Dominguez LJ, Delgado-Rodríguez M. Olive oil consumption and risk of CHD and/or stroke: a meta-analysis of case–control, cohort and intervention studies. Br J Nutr. 2014 Jul 28;112(2):248–59.
- Covas M-I, Nyyssönen K, Poulsen HE, Kaikkonen J, Zunft H-JF, Kiesewetter H, et al. The Effect of Polyphenols in Olive Oil on Heart Disease Risk Factors. Ann Intern Med. 2006 Sep 5;145(5):333.
Salas-Salvadó J, Bulló M, Estruch R, Ros E, Covas M-I, Ibarrola-Jurado N, et al. Prevention of Diabetes With Mediterranean Diets. Ann Intern Med. 2014 Jan 7;160(1):1–10.
Olive oil is a key component of the Mediterranean Diet, being the main source of vegetable fat, especially monounsaturated fatty acids (MUFA). According to the International Olive Council, there are five different types of olive oil: i. Extra Virgin Olive Oil; ii: Virgin Olive Oil; iii: Refined Olive Oil; iv: Olive Pomace Oil and v. Lampante Oil.
Extra Virgin Olive Oil (EVOO) is the best olive oil and it is very precise regards production methods, taste and chemical composition. EVOO must come from the first pressing of fresh olives, normally within 24 hours of harvesting, must be extracted by non-chemical, mechanical means, and without the use of excessive heat, the free fatty acid or acidity level must be less than 0.8% and it must be defect free – having a perfect taste and aroma. It contains multiple bioactive and antioxidant components, such as polyphenols, phytosterols and vitamin E (1). Virgin olive oil also comes from the first pressing and must have an acidity level of less than 2% therefore it is of inferior quality to Extra Virgin Olive Oil. It is flavour intensity can vary and its taste is milder than EVOO.
In contrast, some olive oils are refined by using agents such as acids, alkalis, and heat to extract as much oil as possible from the olive pulp that remains after the first pressing. The result is a fattier and more acidic oil which lacks taste, aroma and natural antioxidants. This is why producers need to add unrefined Extra Virgin or Virgin Olive Oil to impart some of flavour, colour and aroma into the blend. Since refined olive oil during the refining process loses phytochemicals, this oil is mixed with virgin olive oil to enhance the flavour, constituting the so-called common olive oil. The olive – pomace oil is the lowest grade of olive oil and it is made from the by-products of EVOO production. It is bland and extremely low in antioxidants. The lampante oil has severe defects, usually from bad fruit or poor processing practices. It is not fit for human consumption until it has been refined. Finally, the rapeseed oil obtained from canola is one of the oldest known vegetable oil that is also rich in oleic acid, but that differs in several other compounds with common olive oil (2).
Olive oil as a food and the Mediterranean Diet as a food pattern are associated with a decreased risk of cardiovascular disease, obesity, metabolic syndrome, type-2 diabetes and hypertension. A Mediterranean diet rich in olive oil and olive oil per se has been shown to improve cardiovascular risk factors, such as lipid profiles, blood pressure, postprandial hyperlipidemia, endothelial dysfunction, oxidative stress, and antithrombotic profiles. Although some of these beneficial effects can be attributed to the minor components of olive oil, it is very difficult to differentiate the effects of these components from those of the all fruit and even from the effects of the all diet, in this case, the Mediterranean diet (3).
All-cause mortality and cardiovascular mortality: Recent studies consistently support the concept that the OO-rich Mediterranean Diet is compatible with healthier aging and increased longevity. In the PREDIMED (PREvención con DIeta MEDiterránea trial, olive oil consumption, specifically the extra-virgin variety, was associated with reduced risks of cardiovascular disease and mortality in individuals at high cardiovascular risk. For each 10 g/d increase in extra-virgin olive oil consumption, cardiovascular disease and mortality risk decreased by 10% and 7%, respectively (4). Similarly, a lower risk of mortality was associated with regular consumption of olive oil in an Italian population after myocardial infarction and also in an elderly population. In the Spanish cohort of the European Prospective Investigation into Cancer and Nutrition (EPIC) study, total olive oil consumption has been associated with a decreased risk of coronary heart disease, and also all-cause and cardiovascular mortality (5). Thus, there is compiling evidences that olive oil consumption is associated with low all-cause and cardiovascular mortality.
Cardiovascular disease: Evidence suggests that olive oil intake is inversely associated with cardiovascular disease (CVD) in the Spanish general population and in a cohort of Italian women (3). A recent meta-analysis concluded that epidemiologic studies consistently found an inverse association between olive oil consumption and stroke, but there were inconsistencies between studies assessing coronary heart disease (CHD) as the end-point (6). Of note, most of the previous studies made no distinction among the different varieties of olive oil. However, several studies have found a greater beneficial effect in CHD and cardiovascular risk factors for the extra virgin olive oil variety than for the common variety (7). This distinction is important because EVOO contains much higher amounts of polyphenols than common olive oil. These polyphenols may have cardiovascular benefits beyond the lipid profile.
Diabetes: Demonstrated by dietary interventions in different population, olive oil consumption Improvement of glucose metabolism in normal subjects and patients with type 2 diabetes. Substitution of MUFA for SFA results in lower insulin requirement and plasma glucose concentrations, and is at least as effective as CHO. Two prospective studies from Southern European cohorts suggest a lower incidence of diabetes with increasing adherence to Mediterranean Diet in previously healthy persons or survivors of a myocardial infarction. In the PREDIMED trial, the arm of participants who followed a Mediterranean Diet supplemented with extra virgin olive oil showed a 40% reduction in the incidence of diabetes mellitus without significant changes in body weight (8).
Cancer: In countries where the population adheres to the Mediterranean Diet, such as Spain, Greece and Italy, and OO is the principal source of fat, rates of cancer incidence are lower than in northern European countries. Experimental and human cellular studies have provided new evidence on the potential protective effect of olive oil on cancer. Furthermore, results of case-control and cohort studies suggest that MUFA intake including olive oil is associated with a reduction in cancer risk (mainly breast, colorectal and prostate cancers) (4).
Other effects: Olive oil consumption may also have favorable effects on obesity, reduces age-related cognitive decline and incidence of Alzheimer’s disease (4).
In addition, different cohort and intervention studies have observed that olive oil consumption promotes of a less prothrombotic environment compared with SFA-rich diets, influencing different thrombogenic factors: reduction of platelet aggregation, thromboxane B2 production, von Willebrand factor (vWf), tissue factor, tissue factor pathway inhibitor, PAI-1, Factor VII and Factor XII. These latter effects may also help to explain the reduced incidence in myocardial infarction and stroke observed in subjects with higher consumption of olive oil in several cohort studies (4).
References
- Ros E, Hu FB. Consumption of Plant Seeds and Cardiovascular Health. Circulation. 2013 Jul 30;128(5):553–65.
- Bulló M, Juanola-Falgarona M, Hernández-Alonso P, Salas-Salvadó J. Nutritionattributes and health effects of pistachio nuts. Br J Nutr. 2015 Apr 7;113(S2):S79–93.
- Ros E. Nuts and CVD. Br J Nutr. 2015 Apr 7;113 Suppl 2(S2):S111-20.
- Fraser GE, Sabate J, Beeson WL, Strahan TM. A Possible Protective Effect of Nut Consumption on Risk of Coronary Heart Disease. Arch Intern Med. 1992 Jul
1;152(7):1416.
- Aune D, Keum N, Giovannucci E, Fadnes LT, Boffetta P, Greenwood DC, et al. Nut consumption and risk of cardiovascular disease, total cancer, all-cause and cause-specific mortality: a systematic review and dose-response meta-analysis of prospective studies. BMC Med. 2016 Dec 5;14(1):207.
- Guasch-Ferre M, Bullo M, Martinez-Gonzalez MA, Ros E, Corella D, E. R, et al. Frequency of nut consumption and risk of total mortality in the predimed study. Ann Nutr Metab. 2013;62:17–8.
- Zambón D, Sabaté J, Muñoz S, Campero B, Casals E, Merlos M, et al. Substituting walnuts for monounsaturated fat improves the serum lipid profile of hypercholesterolemic men and women. A randomized crossover trial. Ann Intern Med. 2000 Apr 4;132(7):538–46.
- Jenkins DJA, Kendall CWC, Lamarche B, Banach MS, Srichaikul K, Vidgen E, et
- Nuts as a replacement for carbohydrates in the diabetic diet: a reanalysis of a randomised controlled trial. Diabetologia. 2018 Aug 23;61(8):1734–47.
- Casas-Agustench P, López-Uriarte P, Ros E, Bulló M, Salas-Salvadó J. Nuts, hypertension and endothelial function. Nutr Metab Cardiovasc Dis. 2011 Jun;21:S21–33.
- Berryman CE, Grieger JA, West SG, Chen C-YO, Blumberg JB, Rothblat GH, et al. Acute Consumption of Walnuts and Walnut Components Differentially Affect Postprandial Lipemia, Endothelial Function, Oxidative Stress, and Cholesterol Efflux in Humans with Mild Hypercholesterolemia. J Nutr. 2013 Jun 1;143(6):788–94.
Wine is an alcoholic drink made from fermented grape juice. Yeast consumes the sugar in the grapes and converts it to ethanol, carbon dioxide, and heat. Different varieties of grapes and strains of yeasts produce different styles of wine. The effects of wine consumption on health depend on the amount consumed, but also the food with it is consumed. The highest protect effects of wine are reaches when it is consumed in moderation in a healthy diet such as the Mediterranean Diet (1).
Excessive alcohol use is a risk factor for innumerable adverse health outcomes, including cognitive impairment, cancer, cardiomyopathy, cirrhosis, gastrointestinal bleeding, trauma, and social devastation (2). However, several scientific evidences have pointed out that moderate alcohol consumption, especially wine and beer consumption may exert a protective effect on health reducing all-cause, cardiovascular and cancer mortality, as well incidence of cardiovascular disease, diabetes, neurodegenerative diseases and even certain types of cancer (3). The key is the maintenance of a daily moderate consumption of alcohol. The National Institute on Alcohol Abuse and Alcoholism (NIAAA) has defined moderate or low-risk alcohol use as intake of ≤4 drinks on any single day AND ≤14 drinks per week for men and ≤3 drinks on any single day AND ≤7 drinks per week for women (4). Of note, the American Geriatrics Society, NIAAA, and others recommend a limit of 1 drink daily for both men and women aged 65 years and older (5).
The nutritional characteristics of a wine will depend of the type you consider, mainly white or red wine (table 1). The number of calories in wine also depends on the type of wine you choose and the serving size. For example, a serving of red wine is typically five ounces and offers 125 calories. White wine is somewhat lower in calories. Accordingly, the amount of alcohol in the different types of wine also varies significantly between varieties, but the assumption is that wine is 12% ABV (percentage of the drink made up by alcohol). The Table details the main nutritional characteristics of red and white wines according to the USDA (Department of Agriculture of the US Government). The estimated glycemic load of wine is zero. There is no fat, no proteins in wine. However, wine, especially red wine, is very rich in polyphenols, which include a large group of several hundred chemical compounds that affect the taste, colour and mouthfeel of wine. These compounds include phenolic acids, stilbenoids, flavonols, dihydroflavonols, anthocyanins, flavanol monomers (catechins) and flavanol polymers (proanthocyanidins) acids. Finally, wine is also very rich in micronutrients (vitamins and minerals).
Tab.1 – Compositional and Nutritional Characteristics of Red and White Wines (per serving, 147 g wine). Source: Adapted from USDA. Abbreviation: DFE (dietary folate equivalents).
| Nutrient | Red wine | White wine |
| Water (g) | 127 | 128 |
| Energy (kcal) | 125 | 121 |
| Protein (g) | 0.10 | 0.10 |
| Lipid (fat, g) | 0.00 | 0.00 |
| Carbohydrate (g) | 3.84 | 3.82 |
| Total sugars (g) | 0.91 | 1.41 |
| Calcium (mg) | 12 | 13 |
| Iron (mg) | 0.68 | 0.40 |
| Magnesium (mg) | 18 | 15 |
| Phosphorus (mg) | 34 | 26 |
| Potassium (mg) | 187 | 104 |
| Sodium (mg) | 6.0 | 7.0 |
| Zinc (mg) | 0.21 | 0.18 |
| Folate (DFE, μg) | 1.0 | 1.0 |
| Niacin (mg) | 0.329 | 0.159 |
| Riboflavin (mg) | 0.046 | 0.022 |
| Thiamin (mg) | 0.007 | 0.007 |
| Vitamin B6 (mg) | 0.084 | 0.074 |
| Vitamin K (μg) | 0.6 | 0.6 |
Moderate alcohol use is among the most widely studied exposures in the biomedical literature and has been critically reviewed at considerable length by the NIAAA (4). First, epidemiological studies consistently suggest a lower risk of coronary heart disease and myocardial infarction (MI) among moderate drinkers than abstainers. Indeed, the association of moderate alcohol intake appears to be similar among individuals at both low and high cardiovascular risk and even among those with prevalent cardiovascular disease. Of note, a cumulative meta-analysis suggested that our best estimate of the association of alcohol and CHD has not changed in almost 20 years (6).
Different meta-analyses have examined the details of the relationship of alcohol consumption and risk of CHD. In the most quantitative analysis, risk gradually declined until a nadir at 20 gm/day (~1.4 drinks per day) (6). Summary relative risks of approximately 0.8 were found, suggesting that moderate drinking is associated with 20% lower risk of CHD relative to abstention (Figure 1).
In general, the specific type of alcoholic beverage type consumed appears to be less important than the consistency with which alcohol is consumed. The beverage most likely to be inversely related to CHD in a given population tends to be the one most widely consumed in that population. Two systematic reviews of this topic have concluded that beverage type is relatively unimportant, while a recent meta-analysis found higher benefits from wine and beer than from spirits (3). The effect of alcohol on HDL-cholesterol (HDL-C; its major putative mediator) also does not differ by beverage type in controlled experiments. Thus, observational evidence generally supports the hypothesis that it is ethanol intake, per se, that is associated with lower risk of CHD.
Although less well-studied, evidence overall suggests that other coronary outcomes commonly used in clinical trials (e.g., unstable angina, coronary revascularization)
Fig.1. Relative risks of approximately 0.8 were found, suggesting that moderate drinking is associated with 20% lower risk of CHD relative to abstention
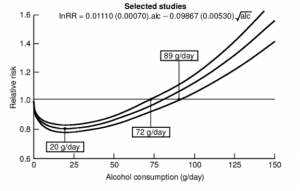
demonstrate similar associations with alcohol as does myocardial infarction. Indeed, several cohort studies have shown similar relationships across all coronary outcomes.
Other cardiovascular outcomes have also been studied extensively in relation to moderate drinking. The association of alcohol consumption with total stroke is complex, given differing associations with the major stroke types of ischemic and haemorrhagic stroke. Of note, it is likely that subtypes within these major types further differ in their associations with alcohol, presumably due to their disparate underlying etiologies. Nonetheless, light-moderate drinking has been associated with a lower risk of ischemic stroke of approximately the same magnitude as for CHD, while haemorrhagic stroke appears to have a dose-dependent positive association with alcohol intake. Etiologically, both effects could reflect an antiplatelet effect of alcohol, with the ascending limb of the J-shape for ischemic stroke further reflecting the role of hypertension due to excessive alcohol intake.
Beyond CHD and ischemic stroke, an increasingly strong series of observational studies now link moderate drinking to lower risk of type II diabetes (7). Meta-analyses suggest that the magnitude of this association might even exceed of CHD, with summary relative risks suggesting ~30% lower risk.
Previous Trials of Alcohol Consumption on Chronic Disease Risk Factors
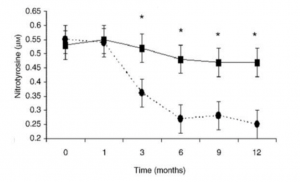
Dozens of trials of moderate drinking over a few weeks have been conducted, many by Dr. Estruch, Hendriks and Shai (8,9). However, very few trials have administered alcohol for more than a few months. Two crossover trials administered alcohol for 16 and 12 weeks, but their design limits their zzz applicability to a long-term RCT. Importantly, a few studies of 3-24 months duration have now been reported. These provide important lessons about the feasibility and design of a long-term randomized trial of alcohol consumption. An Italian group reported a one-year randomized trial of one glass daily of red wine among 115 diabetic survivors of acute MI, although the nature of the intervention was unclear; a specific red wine was recommended, but it is uncertain whether this beverage was actually dispensed. Patients randomized to red wine demonstrated increases in HDL-C and, surprisingly, in echocardiographically determined left ventricular function. Inflammatory markers and insulin resistance also declined. Although biomarkers specific to alcohol were not reported, trends in nitrotyrosine (a short-term marker of oxidative stress) declined throughout the 12 months, suggesting sustained adherence (Figure 1, (10)).
In a 3-month parallel-design trial in Israel comparing wine with a non-alcoholic malt beverage in ~100 non-drinking diabetic adults, Shai et al. found that initiation of wine
Fig. 2. Trends in nitrotyrosine (a short-term marker of oxidative stress) declined throughout the 12 months, suggesting sustained adherence
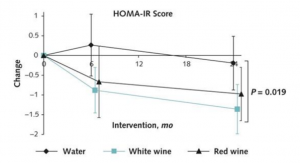
reduced fasting but not post-load glucose. Sleep improved among those randomized to wine, with no other serious side effects. In a ground-breaking follow-up, Shai and colleagues recently reported results of a 24-month-long randomized trial of diabetic adults, assigning individuals to 150 ml of mineral water, white wine, or red wine daily. Among several notable findings, insulin sensitivity improved in both wine groups relative to mineral water, with consistent improvement across the study period (Figure 2). ALT, AST, bilirubin, and alkaline phosphatase did not differ between the 3 groups (9).
Shorter trials of alcohol intake on a variety of secondary outcomes are available and suggest some plausible mechanisms for the effects of moderate drinking. The most compelling results of short-term trials of alcohol intake in humans are on levels of HDL-C. This effect of alcohol has been found so consistently and powerfully that HDL-C now provides a plausible biomarker for alcohol consumption, at least at the population level, and has been used to validate questionnaire-based assessments. A meta-analysis of 36 experimental trials of alcohol administration found that intake of 30 gm/day (i.e., ~2 drinks) raised HDL-C by ~4 mg/dl, an 8% increase from pre-treatment
Fig. 3. Insulin sensitivity improved in both wine groups relative to mineral water, with consistent improvement across the study period
values. As noted, the effect was similar in studies of beer, wine, spirits, or pure ethanol (11).
Short-term trials have also examined the effect of alcohol on measures of glucose metabolism and control. In crossover studies, the USDA found that alcohol consumption had no effect on fasting glucose levels but lowered insulin levels, consistent with improved insulin sensitivity.
Cancer: several non-cardiovascular outcomes have strong, plausible relations with moderate drinking, and these bear directly on the safety of any clinical trial of alcohol consumption. Among these, cancer is the most feared and breast cancer the best studied. In observational studies, alcohol consumption appears to have a linear association with breast cancer, with no safe level of intake. Some evidence suggests a similar relationship for other cancers, although the strongest evidence is for oropharyngeal and esophageal cancers that are less common in the U.S. Perhaps most compellingly, moderate alcohol consumption has been associated with a lower risk of total mortality, chiefly reflecting its inverse association with cardiovascular mortality.
References
- Estruch R, Ros E, Salas-Salvadó J, Covas M-I, Corella D, Arós F, et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet. N Engl J Med. 2013 Apr 4;368(14):1279–90.
- Wang F, Zhang Y-J, Zhou Y, Li Y, Zhou T, Zheng J, et al. Effects of Beverages on Alcohol Metabolism: Potential Health Benefits and Harmful Impacts. Int J Mol Sci. 2016 Mar 9;17(3):354.
- Costanzo S, Di Castelnuovo A, Donati MB, Iacoviello L, de Gaetano G. Wine, beer or spirit drinking in relation to fatal and non-fatal cardiovascular events: a meta-analysis. Eur J Epidemiol. 2011 Nov 11;26(11):833–50.
- Naimi TS, Brewer RD, Mokdad A, Denny C, Serdula MK, Marks JS. Binge drinking among US adults. JAMA. 2003 Jan 1;289(1):70–5.
- AGS Choosing Wisely Workgroup. American Geriatrics Society Identifies Another Five Things That Healthcare Providers and Patients Should Question. J Am Geriatr Soc. 2014 May;62(5):950–60.
- Ronksley PE, Brien SE, Turner BJ, Mukamal KJ, Ghali WA. Association of alcohol consumption with selected cardiovascular disease outcomes: a systematic review and meta-analysis. BMJ. 2011 Feb 22;342:d671.
- Joosten MM, Chiuve SE, Mukamal KJ, Hu FB, Hendriks HFJ, Rimm EB. Changes in Alcohol Consumption and Subsequent Risk of Type 2 Diabetes in Men. Diabetes. 2011 Jan;60(1):74–9.
- Sacanella E, Vázquez-Agell M, Mena MP, Antúnez E, Fernández-Solá J, Nicolás JM, et al. Down-regulation of adhesion molecules and other inflammatory biomarkers after moderate wine consumption in healthy women: a randomized trial. Am J Clin Nutr. 2007 Nov 1;86(5):1463–9.
- Gepner Y, Golan R, Harman-Boehm I, Henkin Y, Schwarzfuchs D, Shelef I, et al. Effects of Initiating Moderate Alcohol Intake on Cardiometabolic Risk in Adults With Type 2 Diabetes: A 2-Year Randomized, Controlled Trial. Ann Intern Med. 2015 Oct 20;163(8):569–79.
- Marfella R, Cacciapuoti F, Siniscalchi M, Sasso FC, Marchese F, Cinone F, et al. Effect of moderate red wine intake on cardiac prognosis after recent acute myocardial infarction of subjects with Type 2 diabetes mellitus. Diabet Med. 2006 Sep;23(9):974–81.
RER Regional law n.28, 28/10/1999 (L.R. n.28, 28/10/1999) [Internet]. [cited 2019 Apr 27]. Available from: http://demetra.regione.emilia-romagna.it/al/articolo?urn=er:assemblealegislativa:legge:1999;28
Herbs and spices have a leading role in Mediterranean Diet, contributing to the well- known flavors and smells related to traditional food preparations like seasonings or traditional sauces, such us pesto. Parsley, oregano, basil, thyme, dill, fennel, marjoram, rosemary, lavender, bay leaf, sage, savory, hyssop cumin and coriander are just few examples of the wide variety of spices and herbs used in Mediterranean Diet. They can be used as colorants, preservatives and they are useful for salt replacement, which have a special interest in the case of people with hypertension and it is a simple, but effective, strategy to reduce salt consumption in also general population.
Herbs and species are relevant by their phytochemicals content that contribute to the organoleptic characteristics and health effects, rather than their contribution at macronutrient level. For instance, bay leaf is flavones-rich food, such as quercetin; kaempferol and coriander seeds are notable by their caffeoyl derivatives and p-coumaric acid content, while leaves are rich in quercetin-3-O-rutinoside (1). Cooking methods also influence spices and herbs composition, that is why the highest phytochemical levels are found in warm liquid and steaming preparations while grilling can reduce their amount and antioxidant capacity (2).
Additionally, herbal extracts have been traditionally used for medical uses by different population, included Mediterranean regions (3). Numerous studies have been conducted in both animals and humans to evaluate herbs and spices effects in health, and it has been found association with benefits over metabolic syndrome, type 2 diabetes, inflammatory level, as well as improvements in blood lipid, glucose levels and blood pressure (4,5). Nevertheless, it is important to continue developing studies in this area, to obtain more robust evidences.
References
- Bhagwat S, Haytowitz DB, Holden JM. USDA Database for the Flavonoid Content of Selected Foods Release 3.1. 2013.
- Chohan M, Forster-Wilkins G, Opara EI. Determination of the Antioxidant Capacity of Culinary Herbs Subjected to Various Cooking and Storage Processes Using the ABTS*+ Radical Cation Assay. Plant Foods Hum Nutr. 2008 Jun 26;63(2):47–52.
- Guarrera PM, Savo V. Wild food plants used in traditional vegetable mixtures in Italy. J Ethnopharmacol. 2016 Jun 5;185:202–34.
- Bower A, Marquez S, de Mejia EG. The Health Benefits of Selected Culinary Herbs and Spices Found in the Traditional Mediterranean Diet. Crit Rev Food Sci Nutr. 2016 Dec 9;56(16):2728–46.
Guldiken B, Ozkan G, Catalkaya G, Ceylan FD, Ekin Yalcinkaya I, Capanoglu E. Phytochemicals of herbs and spices: Health versus toxicological effects. Food Chem Toxicol. 2018 Sep;119:37–49.
Mediterranean Diet include moderate daily intake of dairy products, mainly fermented products such as cheese and yogurt, which traditionally have allowed to preserve milk and to add rich nutrient foods to the diet (1) and have a lower lactose content, but also Mediterranean Diet include milk, which is mostly consumed by children. Cheese, for example, can be eaten alone with bread, added to salads or other culinary preparations, while milk is mainly drunk during breakfast.
Dairy foods are an important source of protein, calcium and vitamin D. In general, these foods are rich in saturated fats so, some guidelines recommend non-fat or moderate low-fat products intake. However, this recommendation it is currently under study.
Dairy foods intake has been related with health effects. Evidence relates fermented food intake in Mediterranean Diet, like cheese and yogurt, with positive microbiome modulation (2,3), in addition these fermented dairy products are associated with lower cardiovascular risk (4,5). Furthermore, a randomized controlled trial, that included old individuals at high risk of cardiovascular disease eating Mediterranean Diet, found that a high daily dairy consumption, especially yogurt, was associated with lower type 2 diabetes risk (6,7), while a high intake of low-fat dairy products, yogurt and low-fat milk were related with a reduction of metabolic syndrome risk. However, there are controversial results about cheese intake and metabolic syndrome risk (8,9). This study also observed that high total dairy intake and low-fat milk consumption in Mediterranean Diet context was related with a lower colorectal cancer risk (10). Nevertheless, more research is needed in this area (11,12).
References
- Bach-Faig A, Berry EM, Lairon D, Reguant J, Trichopoulou A, Dernini S, et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011 Dec 13;14(12A):2274–84.
- Kouris-Blazos A, Itsiopoulos C. Low all-cause mortality despite high cardiovascular risk in elderly Greek-born Australians: attenuating potential of diet? Asia Pac J Clin Nutr. 2014;23(4):532–44.
- Marco ML, Heeney D, Binda S, Cifelli CJ, Cotter PD, Foligné B, et al. Health benefits of fermented foods: microbiota and beyond. Curr Opin Biotechnol. 2017 Apr 1;44:94–102.
- Tapsell LC. Fermented dairy food and CVD risk. Br J Nutr. 2015 Apr 7;113(S2):S131–5.
- de Goede J, Soedamah‐Muthu SS, Pan A, Gijsbers L, Geleijnse JM. Dairy Consumption and Risk of Stroke: A Systematic Review and Updated Dose–Response Meta‐Analysis of Prospective Cohort Studies. J Am Heart Assoc. 2016 May 6;5(5).
- Díaz-López A, Bulló M, Martínez-González MA, Corella D, Estruch R, Fitó M, et al. Dairy product consumption and risk of type 2 diabetes in an elderly Spanish Mediterranean population at high cardiovascular risk. Eur J Nutr. 2016 Feb 7;55(1):349–60.
- Díaz-López A, Bulló M, Martínez-González MA, Corella D, Estruch R, Fitó M, et al. Dairy product consumption and risk of type 2 diabetes in an elderly Spanish Mediterranean population at high cardiovascular risk. Eur J Nutr. 2016 Feb 7;55(1):349–60.
- Babio N, Becerra-Tomas N, Martinez-Gonzalez MA, Corella D, Estruch R, Ros E, et al. Consumption of Yogurt, Low-Fat Milk, and Other Low-Fat Dairy Products Is Associated with Lower Risk of Metabolic Syndrome Incidence in an Elderly Mediterranean Population. J Nutr. 2015 Oct 1;145(10):2308–16.
- Mena-Sánchez G, Babio N, Martínez-González MÁ, Corella D, Schröder H, Vioque J, et al. Fermented dairy products, diet quality, and cardio–metabolic profile of a Mediterranean cohort at high cardiovascular risk. Nutr Metab Cardiovasc Dis. 2018 Oct 1;28(10):1002–11.
- Barrubés L, Babio N, Mena‐Sánchez G, Toledo E, Ramírez‐Sabio JB, Estruch R, et al. Dairy product consumption and risk of colorectal cancer in an older mediterranean population at high cardiovascular risk. Int J Cancer. 2018 Sep 15;143(6):1356–66.
- Lu W, Chen H, Niu Y, Wu H, Xia D, Wu Y. Dairy products intake and cancer mortality risk: a meta-analysis of 11 population-based cohort studies. Nutr J. 2016 Dec 21;15(1):91.
Aune D, Navarro Rosenblatt DA, Chan DS, Vieira AR, Vieira R, Greenwood DC, et al. Dairy products, calcium, and prostate cancer risk: a systematic review and meta-analysis of cohort studies. Am J Clin Nutr. 2015 Jan 1;101(1):87–117.
Mediterranean Diet is rich in legumes (or pulses) intake, like chickpeas, lentils, white beans, broad beans or lupins, among other. They are consumed at least 2 times per week, frequently in stews, soups or as a part of salad.
At nutritional level, legumes intake is a source of vegetable protein, fibre, vitamins, minerals and minority phytochemical compounds.
At nutritional level, legumes intake is a source of plan-based protein, they are low in fat, rich in fibre and contribute with minority phytochemical compounds, which are related to bioactive properties but, at the same time, may have anti-nutritional properties that are eliminated or reduced through processing, soaking, sprouting and fermentation processes. Legumes have a particular interest because are a source of essential amino acids, excluding sulphur containing amino acids, that in combination with other foods represent a good alternative and can substitute red or processed meat and improve diet quality.
Regarding to health, a high legume intake has been associated with health improvements. A meta-analysis that included results from 6 studies and 80,871 incident hypertension cases, concluded that there was an inverse association between legume intake and hypertension risk (1). Moreover, legumes intake has been related to a reduction in total cholesterol and LDL-C (2), so legumes may have a protector role. In addition, high legumes intake has been related to lower obesity and overweight risk (3), and this might be due to a satiating effect, especially in a context of energy restricted dietary patterns (4). Furthermore, gut microbiota legume fermentation leads to the synthesis of short-chain fatty acids, like butyrate, which is a biological interesting compound due to its association with antitumor properties (5,6). In PREDIMED study, a randomized clinical trial, that included old subjects with high cardiovascular risk, found that high legumes intake was associated with lower risk of cancer mortality (7). This study also observed that high legume intake in the framework of Mediterranean Diet was inversely associated with type 2 incidence (8). Legumes can modulate blood glucose levels and contributed to improve insulin sensitivity (9), which is particularly interesting in diabetes treatment (10). Besides, legumes phytochemical compounds are also relevant because of their antioxidant activity (11).
References
- Schwingshackl L, Schwedhelm C, Hoffmann G, Knüppel S, Iqbal K, Andriolo V, et al. Food Groups and Risk of Hypertension: A Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Adv Nutr An Int Rev J. 2017 Nov
15;8(6):793–803.
- Bazzano LA, Thompson AM, Tees MT, Nguyen CH, Winham DM. Non-soy legume consumption lowers cholesterol levels: A meta-analysis of randomized controlled trials. Nutr Metab Cardiovasc Dis. 2011 Feb;21(2):94–103.
- Schlesinger S, Neuenschwander M, Schwedhelm C, Hoffmann G, Bechthold A, Boeing H, et al. Food Groups and Risk of Overweight, Obesity, and Weight Gain: A Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Adv Nutr. 2019 Mar 1;10(2):205–18.
- McCrory MA, Hamaker BR, Lovejoy JC, Eichelsdoerfer PE. Pulse Consumption, Satiety, and Weight Management. Adv Nutr. 2010 Nov 1;1(1):17–30.
- Bird A, Conlon M, Christophersen C, Topping D. Resistant starch, large bowel fermentation and a broader perspective of prebiotics and probiotics. Benef Microbes. 2010 Nov;1(4):423–31.
- Zhu B, Sun Y, Qi L, Zhong R, Miao X. Dietary legume consumption reduces risk of colorectal cancer: evidence from a meta-analysis of cohort studies. Sci Rep. 2015 Aug 5;5(1):8797.
- Papandreou C, Becerra-Tomás N, Bulló M, Martínez-González MÁ, Corella D, Estruch R, et al. Legume consumption and risk of all-cause, cardiovascular, and cancer mortality in the PREDIMED study. Clin Nutr. 2019 Feb;38(1):348–56.
- Becerra-Tomás N, Díaz-López A, Rosique-Esteban N, Ros E, Buil-Cosiales P, Corella D, et al. Legume consumption is inversely associated with type 2 diabetes incidence in adults: A prospective assessment from the PREDIMED study. Clin Nutr. 2018 Jun;37(3):906–13.
- Jenkins DJA, Kendall CWC, Augustin LSA, Mitchell S, Sahye-Pudaruth S, Blanco Mejia S, et al. Effect of Legumes as Part of a Low Glycemic Index Diet on Glycemic Control and Cardiovascular Risk Factors in Type 2 Diabetes Mellitus. Arch Intern Med. 2012 Nov 26;172(21):1653.
- Ramdath D, Renwick S, Duncan AM. The Role of Pulses in the Dietary Management of Diabetes. Can J Diabetes. 2016 Aug 1;40(4):355–63.
Singh B, Singh JP, Kaur A, Singh N. Phenolic composition and antioxidant potential of grain legume seeds: A review. Food Res Int. 2017 Nov 1;101:1–16.
Mediterranean Diet includes a moderate and varied intake of fish (lean fish, oily fish) and shellfish, around 2 or more serves per week. Generally, the variety of the fish consumed depends on the availability, according to sea proximity and the season (cod, sardines, anchovy, mackerel, hake, herring, bluefin tuna, octopus, crustaceans like lobsters and crabs, etc. (1,2)).
Both fish and shellfish are good sources of high-quality proteins and lipids, mainly long-chain PUFA content, especially omega-3 derives such as eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). Although their lipid profile varies significantly among species, saltwater fish have a higher fat content and are richer in omega-3 fatty acids than others (3). Fish is also a good mineral and vitamins source (mainly calcium, iron, selenium, zinc, and vitamin A, B3, B6, B12, E, and D (4)). Nevertheless, it is possible to find certain environmental contaminants, such as heavy metals and organic compounds, in some fish species due to the accumulation along the food chain. For that reason, predatory larger and longest-lived fish may have the highest levels (5).
Polyunsaturated omega-3 fatty acids are present in cellular membrane composition and can participate in gene expression modulation (6,7). They participate in cognitive and retina development and desired omega-3 levels of intake have been associated with beneficial cardiovascular effects (antithrombotic, hypolipidemic, anti-inflammatory and vasodilator (8)). Its intake has been associated with cardiac death prevention by arrhythmia, heart failure and ischemic cardiac events (9). In addition, omega-3-mediated inflammatory response reduction seems to show a protective effect against obesity, metabolic syndrome and type 2 diabetes development, which diseases are characterized by low degree of chronic inflammation (10). Concerning to pollutant levels, a varied diet that includes different fish species prevent a high exposure to these compounds and this is special interesting for frequently fish consumers, pregnant and breastfeeding women and young children (11).
References
- Naimi TS, Brewer RD, Mokdad A, Denny C, Serdula MK, Marks JS. Binge
- Simopoulos AP. Fish and Fish Oil in the Mediterranean Diets. Fish Fish Oil Heal Dis Prev. 2016 Jan 1;15–25.
- Domingo JL, Bocio A, Falcó G, Llobet JM. Benefits and risks of fish consumption: Part I. A quantitative analysis of the intake of omega-3 fatty acids and chemical contaminants. Toxicology. 2007 Feb 12;230(2–3):219–26.
- Sidhu KS. Health benefits and potential risks related to consumption of fish or fish oil. Regul Toxicol Pharmacol. 2003 Dec;38(3):336–44.
- Kris-Etherton PM, Harris WS, Appel LJ. Fish Consumption, Fish Oil, Omega-3 Fatty Acids, and Cardiovascular Disease. Circulation. 2002 Nov 19;106(21):2747-57.
- Gil A, Serra-Majem L, Calder PC, Uauy R. Systematic reviews of the role of omega-3 fatty acids in the prevention and treatment of disease. Br J Nutr. 2012 Jun 17;107(S2):S1–2.
- Corella D, Ordovás JM. Interactions between dietary n-3 fatty acids and genetic variants and risk of disease. Br J Nutr. 2012 Jun 17;107(S2):S271–83.
- Desnoyers M, Gilbert K, Rousseau G. Cardioprotective Effects of Omega-3 Polyunsaturated Fatty Acids: Dichotomy between Experimental and Clinical Studies. Mar Drugs. 2018 Jul 10;16(7).
- Maki KC, Dicklin MR. Omega-3 Fatty Acid Supplementation and Cardiovascular Disease Risk: Glass Half Full or Time to Nail the Coffin Shut? Nutrients. 2018 Jul 4;10(7).
- Tortosa-Caparrós E, Navas-Carrillo D, Marín F, Orenes-Piñero E. Anti-inflammatory effects of omega 3 and omega 6 polyunsaturated fatty acids in cardiovascular disease and metabolic syndrome. Crit Rev Food Sci Nutr. 2017 Nov 2;57(16):3421–9.
Gil A, Gil F. Fish, a Mediterranean source of n -3 PUFA: benefits do not justify limiting consumption. Br J Nutr. 2015 Apr 7;113(S2):S58–67.
Although Mediterranean Diet is mainly a plant-based dietary pattern, it also includes moderate intake of lean meat, such as poultry and eggs, while red and processed meat intake is limited (1). Eggs, for instance, are used as the main ingredient in some traditional recipe preparations.
Lean meat and eggs are high quality protein, mineral and vitamin sources. Lean meat composition is based on lower saturated fatty acids levels compared to non-lean meats, while eggs composition is rich in monounsaturated fatty acids and cholesterol (2).
Lean meat intake instead of red or processed meat is more beneficial, especially in the prevention of some diseases which a high intake of red and processed meat has been associated to a higher risk: metabolic syndrome, type 2 diabetes, cardiovascular diseases, and some kinds of cancer (3-6). In fact, processed meat has been recently classified as carcinogenic agent and red meat as a probably carcinogenic agent by the International Agency for Research on Cancer (IARC) from the World Health Organization (WHO, (7)).
The association between eggs and health has been widely discussed, mainly because of their high cholesterol content. Last published results suggest that egg intake is associated to total cholesterol (TC) blood plasma, LDL-C and high-density lipoprotein cholesterol (HDL-C) increase, but without effect over triglycerides concentration or LDL-C/HDL-C and TC/HDL-C ratios (8). However, regarding cardiovascular diseases risk and eggs intake link, there appears not to be enough scientific evidence that support this association, however in patients with cardiovascular diseases and/or type 2 diabetes a moderate intake would be prudent (9,10). Nevertheless, controversies remain in this field and more research is necessary.
References
- Bach-Faig A, Berry EM, Lairon D, Reguant J, Trichopoulou A, Dernini S, et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011 Dec 13;14(12A):2274–84.
- Food Composition Databases Show Foods List [Internet]. [cited 2019 Apr 15]. Available from: https://ndb.nal.usda.gov/ndb/search/list
- Becerra-Tomás N, Babio N, Martínez-González MÁ, Corella D, Estruch R, Ros E, et al. Replacing red meat and processed red meat for white meat, fish, legumes or eggs is associated with lower risk of incidence of metabolic syndrome. Clin Nutr. 2016 Dec 1;35(6):1442–9.
- Kouvari M, Notara V, Kalogeropoulos N, Panagiotakos DB. Diabetes mellitus associated with processed and unprocessed red meat: an overview. Int J Food Sci Nutr. 2016 Oct 2;67(7):735–43.
- Micha R, Wallace SK, Mozaffarian D. Red and Processed Meat Consumption and Risk of Incident Coronary Heart Disease, Stroke, and Diabetes Mellitus. Circulation. 2010 Jun 1;121(21):2271–83.
- Larsson SC, Wolk A. Meat consumption and risk of colorectal cancer: A meta-analysis of prospective studies. Int J Cancer. 2006 Dec 1;119(11):2657–64.
- IARC Monographs evaluate consumption of red meat and processed meat. 2015.
- Rouhani MH, Rashidi-Pourfard N, Salehi-Abargouei A, Karimi M,
- Haghighatdoost F. Effects of Egg Consumption on Blood Lipids: A Systematic
- Review and Meta-Analysis of Randomized Clinical Trials. J Am Coll Nutr. 2018 Feb 17;37(2):99–110.
- Geiker NRW, Larsen ML, Dyerberg J, Stender S, Astrup A. Egg consumption, cardiovascular diseases and type 2 diabetes. Eur J Clin Nutr. 2018 Jan 27;72(1):44–56.
- Shin JY, Xun P, Nakamura Y, He K. Egg consumption in relation to risk of cardiovascular disease and diabetes: a systematic review and meta-analysis. Am J Clin Nutr. 2013 Jul 1;98(1):146–59.
At present, there are many sources of information that provide advice on nutrition and how the population should be fed, and sometimes, this creates confusion, because each country has different cultures, and this is difficult to adapt. That is why the dietary guidelines are an important part of promoting the consumption of adequate food within each sector of the world’s population.
The food guides are the educational tool that the health administrations make available to the general healthy population in order to adapt in an easy and understandable way the scientific knowledge about the nutritional requirements and food composition. They are shown graphically and easy to understand. Almost all countries have a guide, designed according to the policies that govern it. It is considered a very useful tool to educate and guide the population towards a healthier diet. They are extremely important because they influence the promotion of health and thus prevent diseases that are increasing today. They are also adapted in relation to the culture, customs, and availability of food for each of them.

Albania
Recommendations on healthy nutrition in Albania (Albanian: Rekomandime për një ushqyerje të shëndetshme në Shqipëri) (22)
Executing entities:
- Institute of Public Health,
- Ministry of Health – Draft Stability Pact on the Strengthening of Food Security and Nutrition Services in the Southeast Countries,
- Health Sector,
- Food quality sector,
- Ministry of Agriculture,
- Food and Customer Protection,
- Ministry of Education and Science,
- Directorate of Public Health,
- Center for Economic Education and the Growth of Children in the Municipality of Tirana.
Supporting entities: –
Year of publication: 2008
Language: Albanian and English
Format: Report
Graphic representation: Pyramid
Validation: Pending

Bosnia and Herzegovina
Guide on nutrition for the adult population (Bosnian: Vodič o ishrani za odraslu
populaciju) (23)
Executing entities:
- Institute of Public Health,
- Federation of Bosnia and Herzegovina,
- Federal Ministry of Health,
- Federal Ministry of Education,
- Non-governmental organization,
Supporting entities: –
Year of publication: 2004
Language: Bosnian
Format: Report
Graphic representation: Round pyramid
Validation: Pending

Croatia
Dietary guidelines (Croatian: Prehrambene smjernice) (24)
Executing entities:
- Ministry of Health,
- Ministry of Education,
- Croatian Institute of Public Health,
- Clinical hospitals.
Supporting entities: –
Year of publication: 2002
Language: Croatian
Format: Report
Graphic representation: Pyramid
Validation: Pending

Cyprus
National nutrition and exercise guidelines (Greek: εθνικές οδηγίες διατροφής και άσκησης) (25)
Executing entities:
- Ministry of Health,
- Ministry of Education,
- Consumer and nutrition associations,
- Non-governmental organizations.
Supporting entities: –
Year of publication: 2007
Language: Greek
Format: Report
Graphic representation: Pyramid
Validation: Pending

Greece
Dietary guidelines for adults in Greece (26)
Executing entities:
- Supreme Scientific Health Council,
- Hellenic Ministry of Health.
Supporting entities: –
Year of publication: 1999
Language: Greek and English
Format: Website
Graphic representation: Pyramid
Validation: Pending

Italy
Guidelines for healthy Italian food habits, 2003 (Italian: Linee guida per una sana
alimentazione italiana. Revisione 2003) (27)
Executing entities:
- Istituto Nazionale di Ricerca per gli Alimenti e la Nutrizione,
- Istituto Superiore di Sanità,
- Università di Parma,
- Università La Sapienza,
- Università di Bologna,
- Ospedale S. Filippo Neri,
- Università di Milano,
- Università di Padova,
- WHO Politiche Nutrizionali,
- Ospedale Bambin Gesù,
- Università di Napoli,
- Universtà di Ferrara,
- Università della Tuscia.
Supporting entities: –
Year of publication: 2003
Language: Italian
Format: Report
Graphic representation: No
Validation: Pending

Portugal
A nova roda dos alimentos – 2015 (28)
Executing entities:
- Faculdade de Ciências da Nutrição e Alimentação da Universidade do Porto.
Supporting entities:
- Instituto do Consumidor,
- Faculdade de Ciências da Nutrição e Alimentação da Universidade do Porto,
- Associação Portuguesa de Nutricionistas
Year of publication: 2015
Language: Portuguese
Format: Poster
Graphic representation: Wheel (plate)
Validation: No
Other information: The Food Wheel emerged in 1977 during the campaign «Know how to eat is to know how to live» and in 2003 it was restructured due to the evolution of scientific knowledge and the clear alteration of the alimentary habits of the Portuguese. This project was developed within the framework of the Health XXI program, through a protocol between the Faculty of Nutrition and Food Sciences of the University of Oporto and the Consumer Institute. In this way, some of the groups were subdivided and water was added.

Slovenia
12 steps to healthy eating (Slovene: 12 korakov do zdravega prehranjevanja) (Nacionalni Institut Za Javno Zdravje, 2011; Priporočila Za Zdravo Prehranjevanje, 2009) (29)
Executing entities:
- National Institute of Public Health,
- WHO CINDI,
- Program (Integrated Intervention of Integrated Noncommunicable Diseases in Slovenia) in Slovenia Experts.
Supporting entities: –
Year of publication: 2009
Language: Slovenian
Format: Report and poster
Graphic representation: Pyramid
Validation: Search
Other information: Slovenia’s dietary guidelines «12 steps to healthy eating» were published in 2000 and revised in 2011. The «food pyramid» (Slovenian: Z zdravo prehrano in gibanjem do zdravja) was published in 2000 and revised in 2015. » (Slovenian: Zdrav krožnik) was published in 2007.

Spain
Dietary guidelines for the Spanish population; the new pyramid of healthy eating (30)
Executing entities:
- Spanish Society of Community Nutrition (SENC).
Supporting entities:
City Council of Guadix; Behavioral Sciences Institute; CEU-San Pablo-Hospitals of Madrid; CiberOBN; Dieticians Association of Andalusia; Ministry of Health, Community of Madrid; Consellería de Sanitat, Generalitat Valenciana; Departament de Sanitat, Generalitat de Catalunya; FINISH; FIDEC Foundation- UPV / EHU; Nutritional Research Foundation; Jiménez Díaz Foundation; Clinical Hospital of Madrid; Hospital La Paz-Madrid; Virgen del Rocío Hospital-Seville; IMIM-CIBERESP; Carlos III Health Institute; Nutrition without Borders; SEMER; SEMERGEN; SemFYC; SENC; SEPEAP; CEU-San Pablo University; Complutense University; University of Barcelona; Cadiz University; University of Granada; University of the Balearic Islands; University of Las Palmas de Gran Canaria; University of Leon; University of Navarra; Sevilla University; University of Valladolid; University of the Basque Country, UPV-EHU; Open University of Catalonia; polytechnic university of Valencia; Ramón Llull University; Rovira i Virgili University
Year of publication: 2016
Language: Spanish
Format: Report
Graphic representation: Pyramid
Validation: No
Other information: The Working Group of the Spanish Society of Community Nutrition (SENC) to update the Dietary Guidelines for the Spanish population has been working in the last two years in the review of scientific evidence as a basis for updating the Dietary Guidelines. He has considered the most frequent health problems with a focus on public health, the most prevalent eating habits, as well as the practice of physical activity and sedentary lifestyle in the Spanish population. It has also taken into account the current socio-economic context and relevant cultural factors.
An important part of the review process has been the involvement of consumers, considering their contributions and points of view. Other sectors have also been involved. Our recognition of the work, contributions, comments and involvement of all scientists, citizens and professionals who have collaborated in this initiative.

Mediterranean countries
Mediterranean Diet Pyramid: a current lifestyle. Guide for the adult population (2010)
Executing entities:
- Fundación Dieta Mediterránea
Supporting entities:
- International Commission on the Antropology of Food and Nutrition; Red-Predimed; Universitat Politécnica Delle Marche; Centro Interuniversitatio Internazionale di Studi sulle Culture Alimentari Mediterranee; Hellenic Health Foundation; International Union of Nutritional Sciences; Hebrew University – Hadassah Braun School of Public Health & Community Medicine; International Centre for Advanced Mediterranean Agronomic Studies; Federation of African Nutrition Societies; Federation of European Nutrition Societies.
Year of publication: 2010
Language: Arab, Spanish, Catalan, Euskera, French, Galician, Greek, English, Italian, Portuguese.
Format: Article
Graphic representation: Pyramid
Validation: No